

The connection between workforce deployment and patient safety is paramount in healthcare. Exploring the role of our safety solutions along with the human factors and the consequences of culture and behaviours across organisations on patient care made me consider how our connected solutions in SafeCare and Datix actually support in a day-to-day practical way?
I often get asked about Red Flags. Red flags highlighted in SafeCare are our first signal that there is a potential for harm occurring.
A Red Flag is NOT an incident; indeed, their purpose is the AVOIDANCE of Incidents.
How did they come about? The National Institute for Health and Care Excellence (NICE) guidelines for Safe Staffing for nursing in adult inpatient wards in acute hospitals (2014), recommended red flags, specifically attributable to nursing workforce.
These have since been a consistent framework to assess if clinical staff available on the day meet patients’ needs and to highlight any subsequent risk associated with the workforce deployment as it becomes evident. It’s really important to remind ourselves about exactly what constitutes a red flag as the temptation to broaden the scope can easily snowball to a blur of varying degrees of normality to a serious potential for harm.
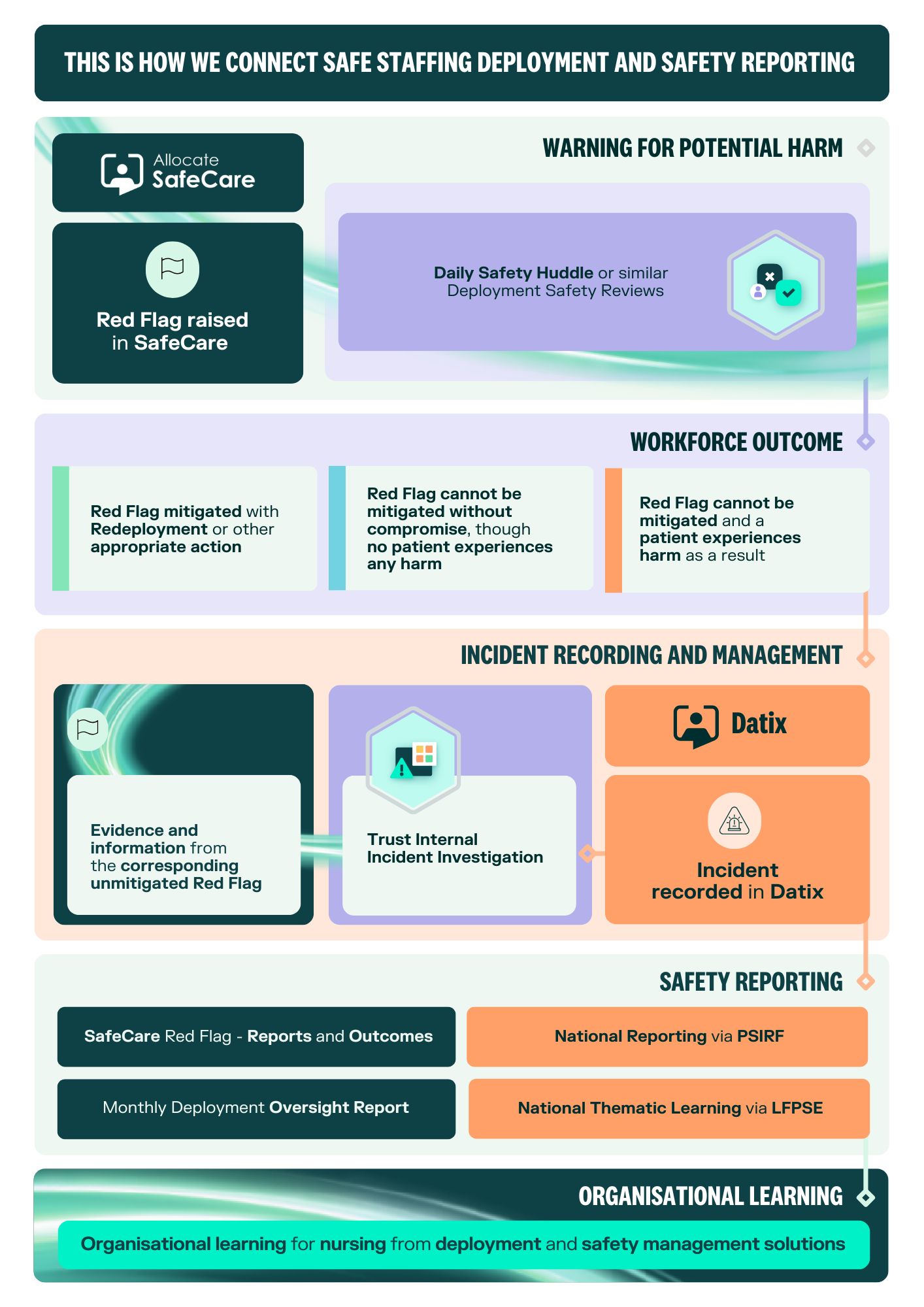
Therefore, Red Flags offer an early warning that there is a potential for harm to occur as a result of the clinical workforce allocation and therefore an opportunity to mitigate and divert the associated risk, through redeployment or an alternative action. When inputting red flags, they are assigned to an owner. This person should be responsible for monitoring or actioning any requirements to solve the flagged issue as well as to ensure it is marked as such and closing when resolved. This live solution offers the opportunity to mitigate the risk highlighted and as such, ensuring that no patient experiences harm.
The monitoring of their occurrence should be undertaken throughout each 24-hour period and records of them maintained for learning purposes and to inform future planning of ward nursing staff establishments. As a benchmark, an average of 105-115 Red Flags are raised across an organisation in each 24 hours. In practical terms most of this early reporting, mitigation monitoring and learning will often take place in the daily safe staffing huddles.
To track the use of Red Flags and any ongoing improvements and learning we would recommend using the reporting process in SafeCare – Red Flags- Search Red Flags. This report will show the type, date, owner and status of red flags made. The recombination would be to run the report with the status of ‘All’ to see the total made and ‘Open’ to see what is outstanding and / or ‘Closed’ to see the total mitigated with actions and changes made to the nursing workforce deployment.
Should a Red Flag not be able to be mitigated and as a result, harm occurs to a patient, then an Incident is then created and documented as such in Datix. In such circumstances, then the investigation may seek to retrieve the associated evidential documentation from SafeCare as to the workforce situation at the time of the incident or leading up to the incident occurring. This of course will be one part of a complex investigation but a vitally important factor to be included.
Ultimately the governance and reporting opportunities from these systems and solutions pertaining to workforce deployment, operational activity, risk and incident reporting, collectively offer identifiable learning opportunities for improvement. Patient safety must be at the forefront of all our minds, with solutions which can afford consistent processes for highlighting and recording risk and safety incidents and offer supportive evidence to investigative procedures.
The intrinsic link between workforce and patient safety is well recognised and the more tangible and visible the evidence of this across our healthcare systems, can only improve care outcomes for our patients.

Clinical Lead, RLDatix
Karen’s career has spanned both the NHS and Criminal Justice, with senior leadership roles that have delivered improvements at organisational, regional, and national levels, enhancing patient care and work environments. These improvements have involved safe staffing, clinical practice, technology, and workforce management. Prior to joining RLDatix Karen was Head of Nursing Clinical Workforce Productivity at NHS England.



